Abstract
Background:A Nosocomial infection is an infection which was not present or was in the
incubation period at the time the patient is admitted to the hospital, but occurs within 72
hours after admission. They are potentially caused by organisms that are resistant to
antibiotics. Highest prevalence of nosocomial infections is found in intensive care units
and also it is one of the leading causes of death in intensive care units.
.
Aims: To describe the prevalence of nosocomial infections and describe the types and
distribution of associated factors of nosocomial infections in the intensive care setting of
Colombo North Teaching Hospital, Sri Lanka.
.
Methods:
A descriptive cross sectional study was conducted among patients admitted to
the Intensive Care Unit of Colombo North Teaching Hospital for one year duration from
August 2015. Patients who did not have fever spikes 48 hours before the admission were
included. Systematic random sampling technique was applied. Data collection was done
by using an Interviewer Administered questionnaire and analyzed by SPSS 23.0 statistical
software. 95% confidence interval was taken for statistical significance.
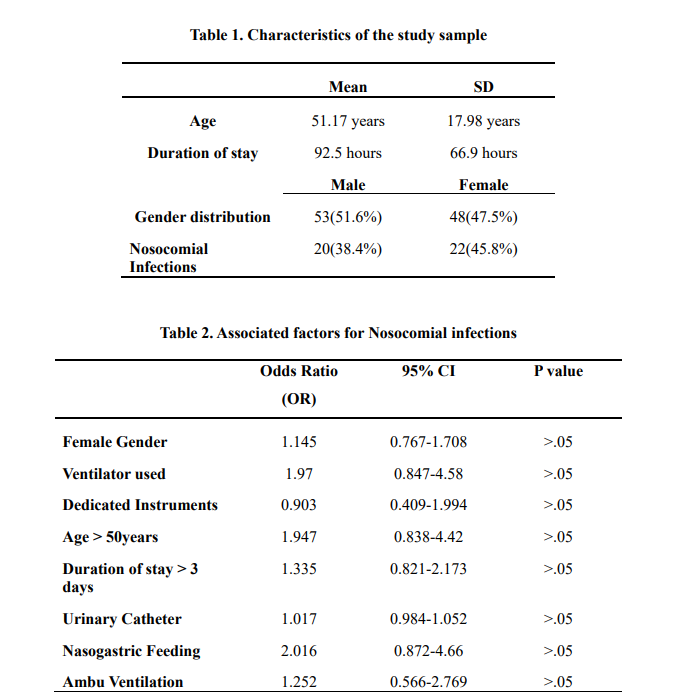
Results: Prevalence of nosocomial infections in the study sample was 41.58% (N= 42).
This male predominant study sample (51.6%), showed a normal distribution of age which
ranged from 9 years to 83 years (Mean=51.17: SD=17.98). Acquiring infections did not
depend on the sex of the patient. (OR=0.767; 95% CI=0.347-1.695). Mechanical
ventilation was identified as a risk factor for acquiring nosocomial infections (OR=1.97;
95 CI%= 0.847-4.58). Using dedicated instruments was identified as a protective measure
for nosocomial infections (OR=0.903:95%: CI=0.409-1.994). Risks identified for
acquiring nosocomial infections include age above 50 years (OR=1.947:95%: CI=0.838-
4.42) and more than three days stay at the intensive care unit (OR=1.335:95%: CI=0.82-
2.173)..
Conclusion
Except using dedicated instruments all the associated factors considered in
the study were identified as risk factors for nosocomial infections. Using dedicated instruments was recognized as a protective factor for nosocomial infections. Duration of
intensive care unit stay and the treatment procedures directly affected the spreading of
nosocomial infections. As morbidity and mortality trends of the patients are remarkably
increased with nosocomial infections, it is essential to suppress the associated factors and
minimize the spread of nosocomial infections.
Key Words: Infections, Nosocomial, Intensive Care
Introduction
The term "Nosocomial" comes from two
Greek words; "nosus" meaning "disease"
and "komeion" meaning "to take care
of." Hence, "Nosocomial" is applied to
any disease contacted by a patient while
under medical care. However, the term
hospital-acquired is used synonymous
with the word "Nosocomial"
(1). A
Nosocomial infection is an infection
which was not present or was in the
incubation period at the time the patient
is admitted to the hospital, but occurs
within 72 hours after admitting to the
hospital. They are potentially caused by
organisms that are resistant to
antibiotics
(2).
Despite the rapid progress in facilities
and hospital care, infections continue to
develop in hospitalized patients, and
may also affect the hospital staff. Many
factors promote infection among
hospitalized patients. These will be
include pathophysiological conditions of
the patient and poorly maintained
hospital environment which facilitates
transmission of infection.
Most frequently identified Nosocomial
infections are infections of surgical
wounds, urinary tract infections and
lower respiratory tract infections. The
WHO study and other studies have
shown that the highest prevalence of
Nosocomial infections is found in intensive care units and in acute surgical
and orthopaedic wards. Hospital-acquired infections add to
functional disability and emotional stress
of the patient and in some cases may lead
to disabling conditions that reduce the
quality of life. Nosocomial infections are
also one of the leading causes of death.
The economic cost is also important.
Increased length of stay of the infected
patient contributes mainly to increased
cost. In 2014, there were 707 deaths and
death rate in ICU was 13.5(IMMR 2012)
Cause of death in ICU patients were not
among published data. Detailed
investigation of Nosocomial infections
and its causative factors are essential for
future planning as well as for resource
allocation to minimize the burden of
Nosocomial infections to the country.
Teaching hospitals have a large turnover
of patients as most of the critical patients
are transferred to them from peripheries
and relatively large number of ICU beds
are available at teaching hospitals.
(3)Objectives of the study were to describe
the prevalence of Nosocomial infections
and describe the types and distribution of
associated factors of nosocomial
infections in the Intensive Care setting of
Colombo North Teaching Hospital, Sri
Lanka.
Methodology
A descriptive Cross sectional study was
conducted among patients admitted to
Intensive Care Unit of Colombo North
Teaching Hospital for one year duration.
Patients admitted to the ICU for more
than 24 hrs and patients who did not have
fever spikes 48 hrs before the admission
were included to the study. Patients who
developed fever spikes within 48 hrs of
admission were excluded. Sample size
was calculated by using Lwanga and
Lemeshow equation and it was 101
(4).
Systematic random sampling technique
was applied for sample selection.
Data collection was done by using an
Interviewer Administered data sheet at
the Intensive Care Unit. Data were
collected at an interview with the patient
and extracts from BHTs. Data were
analysed by SPSS 22.0 statistical
software. 95% confidence interval was
taken for statistical significance.
Administrative clearance was obtained
from the Director of the Hospital and the
Consultants in charge of the ICU. This
project was ethically cleared by ERC
faculty of Medicine Ragama, Sri Lanka.
.
Results
Prevalence of Nosocomial infections in
the study sample was 41.58% (N= 42).
There were 51.55 (N=52) of males and
47.5% (N=48) of females in the study
sample. Age showed a normal
distribution which ranged from 9 years
to 83 years (Mean=51.17: SD=17.98).
Patients admitted to Intensive Care Unit
were treated for 24 hours to 408 hours.(Mean 92.5hrs:SD=66.9hrs) Acquiring
Infections did not depend on sex of the
patient. (OR=0.767:95% CI =0.347-
1.695).
Although mechanical ventilation was
identified as a risk factor for acquiring
Nosocomial infections (OR=1.97), it did
not show a significant effect (95
CI%=0.847-4.58). Using dedicated
instruments was identified as a
protective measure for preventing
Nosocomial Infections (OR=0.903). But
it did not show significant figures(95%
CI=0.409-1.994).Age above 50 years is
considered as a risk factor for
nosocomial infections (OR=1.947:95%
CI=0.838-4.42). A high risk of acquiring
nosocomial infections was identified in
patients who had an Intensive Care Unit
stay for more than three days
(OR=1.335:95%CI=0.82-2.173).
Urinary catheterization (OR=1.017:95%
CI=0.984-1.052), nasogastric feeding
(OR=2.016:95% CI=0.872-4.66), and
Ambu ventilation (OR=1.252:95%
CI=0.566-2.769) were identified as
positive contributors for Nosocomial
Infections. Out of all associated factors,
nasogastric feeding showed the highest
odds ratio (2.016). Except using
dedicated instruments all the associated
factors considered in the study were
identified as risk factors for nosocomial
infections. Using dedicated instruments
was recognized as a protective factor for
preventing nosocomial infections.
Discussion
Predominant risk factors identified for
acquiring nosocomial infections during
an Intensive care unit stay are
mechanical ventilation, Naso Gastric
feeding, central venous line insertion and
age above 50years. Although the risk of
spreading nosocomial infections can be
minimized by using dedicated instruments for each and every patient, it
is not practical to practice such isolation
in a very busy Intensive Care setup. But
dedicated instruments can be used with
minimum expenses when a single set of
instruments are used for a single patient
until the patient is discharged from the
Intensive Care Unit. Several
confounding factors such as low
immunity, medical comorbidities and nutritional imbalances could affect the
increased risk of acquiring Nosocomial
Infections among patients with a higher
age. Exposure to microorganisms is
significantly high and immunity status is
diminished in prolonged Intensive Care
Unit stay. Therefore risk of acquiring
infection is increased with increased
Intensive Care Unit stay, especially the
instruments can be easily contaminated
with biological secretions. Therefore
using dedicated instruments during
prolonged Intensive Care Unit stay helps
to minimize microorganism
transmission.
Possibility of developing nosocomial
infections at critical care settings in
developed countries is 30% .
(5). But this
value is expected to be doubled among
the developing countries. Age above 65
years is identified as a risk factor for
nosocomial infections. Nasogastric
nutrition, Central Venous line insertion
and urinary catheterization are identified
and proven risk factors for nosocomial
infections by several studies. Prolonged
Intensive Care Unit stay more than ten
days is identified as a risk factor for
nosocomial infections in developed
countries.
(6). But during this present
study, Intensive Care Unit stay more than
three days was observed as a risk factor
for nosocomial infections.
Association of sociodemographic factors
was not studied during the study and
ethnic and religious factors, occupational
and social status should be considered as
well. Reasons for Intensive Care Unit
admission and the confounding effects
created by comorbidities of the
participants were not addressed during
the study.
Outcome variable which was used in the
study was the incidence of nosocomial
infections and it was defined by
recording the fever episodes above normal body temperature. They were not
confirmed by culture studies. Raised
body temperature could be a result of
many other pathologies apart from
nosocomial infections. Reliability of the
study becomes questionable due to
above reasons and it causes reduction of
internal and external validity.
A patient is admitted to an Intensive Care
Unit when his life is in a critical stage
and the aim is to make necessary
treatment methods and minimize the risk
and discharge from the Intensive Care
Unit as soon as possible. If a patient
happens to acquire new infections from
an Intensive Care Unit it will prolong his
ICU stay and will aggravate his critical
situation.
Conclusion/Recommendations
Anyhow the associated risk factors and
protective features identified in this
study should be studied in detail
especially with a larger sample size and
with a study design that minimizes
confounding effects. A well-defined
matched case control study design can be
recommended for future studies.
It is essential to implement new practical
methods to minimize Nosocomial
Infections which generate many adverse
effects. So practical implementation
procedures for using dedicated
instruments should be established and
their feasibility has to be studied in
detail.
Intensive Care Unit admitted patients
acquire Nosocomial Infections more
frequently. Duration of Intensive Care
Unit stay and the treatment procedures
done at the Intensive care unit directly
affect the spreading of Hospital Acquired
Infections. As patients’ morbidity and
mortality trends are remarkably
increased with Nosocomial Infections it
is essential to suppress the associated factors and minimize the spread of
Nosocomial Infections. Feasibility of
low cost methods in minimizing
Nosocomial Infections should be studied
in detail. .
References
1.Kouchak F, Askarian M. Nosocomial Infections: The Definition Criteria. Iran J
Med Sci [Internet]. 2012 Jun;37(2):72–3; Available from
2. Ministry of Health Sri Lanka. Anual Health Bulleting 2015. 2015.
3. Lwanga SK LS 1991. Sample size determination in health studies: A practical
manual. Geneva.: World Health Organization; 1991.
4.G. Ducel, J. Fabry LN. Prevention of hospital-acquired infections. World Heal
Organ [Internet]. 2002;1–64. Available from
5.Yesilbağ Z, Karadeniz A, Başaran S, Kaya FÖ. Nosocomial infections and risk
factors in intensive care unit of a university hospital. J Clin Exp Investig
[Internet]. 2015;6(3):233–9.. Available from
6.WHO. Practical Guidelines for Infection Control in Health Care Facilities
Practical Guidelines for Infection Control in Health Care Facilities. World Heal
Organ [Internet]. 2004;110. .Available from