Abstract
Background: Congenital Heart diseases are the commonest congenital disease in the
world. It requires regular frequent monitoring and necessary adaptations of the life style.
Although the clinic services are free for a child with Congenital Heart Disease, attending
the clinic generates a significant amount of out of pocket expenses; studying them and
associated factors is a timely need.
Aims: To describe the Socio-demographic characteristics of families that owns a child
less than 5 years of age with congenital heart disease and calculate the out of pocket
expenditure of those families for a clinic visit.
Methods:
A descriptive cross sectional study was conducted among 335 children from
September to November 2014. Systematic random sampling technique was applied with
an interviewer administered structured questionnaire. Data was analyzed by using SPSS
version 23.0
Results: There was a Sinhala Buddhist female predominance, (53.4%) which was not
significant. Majority of them were from the central province and were diagnosed during
their infancy. Ages of the children varied between 12 to 60 months (Mean37.1:SD14.5).
Among them the most common (40.3%) congenital heart disease was Mitral Valve
Prolapse (N=135). Twenty three percent of participants had taken support from outside
people to attend the clinic but no one had to pay for them. Majority (80.9%) of employed
parents could not attend to work on the clinic day and 23% of participants lost their daily
income due to the clinic visit. Total income of the families varied from Rs.12,000/= to
Rs.80,000/= (Mean=Rs.23759.7: SD=Rs.9026.6). Mean expenditure for clinic visit was
Rs1246/= (SD=Rs.650.8). Expenses were not associated with the age (p>0.05), type of
the CHD (p>0.05), or gender (p>0.05).
Conclusion
Reducing the period of stay at the clinic by allocating a specific time and
providing an efficient service during that time can be used to minimize the expenses for
food lodging and transport. This study can be expanded to calculate then on-medical out
of pocket expenses when undergoing a corrective surgery. The psychological effects
generated on a congenital heart disease child when living with the limitations of life
should be studied in detail.
Key Words: Heart Diseases, Congenital, Expenses
Introduction
Congenital Heart Diseases (CHD) are
the commonest congenital abnormality
found in the world and in Sri Lanka
(1).There are several types of Congenital
Heart Diseases and they are distributed
in many countries in different
geographical areas among different
social groups. This distribution may
associate with many factors, which are
worth studying mainly to evaluate the
disease burden to a country. The direct
cause for CHD is unknown although
there are related factors such as genetic
disorders, consanguinity, maternal
infections.
(2) But, risk factors or causes
are not identified for a considerable
amount of patients. So, the associated
factors such as sociodemographic,
economic, environmental and cultural
exposures should be investigated in
detail and should be shared in several
settings. This can be used to understand
multiple associations in order to develop
a hypothesis to establish the causative
factors.
Sri Lanka, as a country which provides
free health care facilities for the whole
population, bears the health care
expenses of children with congenital
heart defects as well. But as the services
are not at the door step level, people have
to reach certain specialized institutions
to get services. Visiting these institutions
from faraway places in a regular frequent
manner to get the essential and required treatment, obviously causes a great
burden to the whole family.
In Sri Lanka, estimated number of live
births with a congenital heart defect for a
single year is 3024
(3). Although they
are scattered all over the country, there
are very limited number of paediatric
cardiology clinics functioning at present.
Patients face unlimited number of
difficulties while attending these clinics
and the clinic at Sirimavo Bandaranaike
Specialized Children’s Hospital
Peradeniya gives services to patients
from several provinces of the country.
Although all the treatment expenses of a
congenital heart disease patient are spent
by the government via hospital clinic,
there can be many opportunities for
additional expenses during clinic visits
and many other associated events. These
expenses are called out of pocket
expenses and studying and analysing
these expenses with sociodemographic
characteristics of families, were the aims
of this study.
Methodology
A descriptive cross sectional hospital
based study was conducted at Sirimavo
Bandaranaike Specialized Children’s
Hospital Peradeniya.Study was
conducted for a period of six months
from November 2014 to April 2015,
after obtaining ethical clearance from the
Ethical Review Committee Faculty of
Medicine, Colombo. Children under 5 years attending the Paediatric
Cardiology Clinic at the SBSCH
Peradeniya during the study period, were
considered as the study population.
Children diagnosed with a congenital
heart disease, presented with a diagnosis
card and children less than five years of
age were included to the study. Children
with co-existing other congenital
abnormalities, children attending the
cardiology clinic due to any other reason
other than the routine clinic visit,
children who have undergone cardiac
surgeries and children presenting with
any other illness on the visiting day such
as Respiratory tract infections and
Urinary Tract Infections were excluded.
Sample size was calculated by using the
Lwanga & Lemeshow equation
(4) and it
was 335. Systematic sampling technique
was applied to obtain the required
sample size. An interviewer
administered structured questionnaire
was used for data collection.The
Questionnaire was prepared in English
and was translated to Sinhala and Tamil.
Questions consisted of both open and
close ended questions. The questionnaire
consisted of three parts; socio
demographic characteristics of the child,
information regarding the congenital
heart disease and information required to
calculate the out of pocket expenditure
for a clinic visit. Questionnaire was
developed after extensive literature
review and with the contribution of
many expert ideas of several specialities
in the subject stream. Data sheet was not
validated, but was pretested one month
prior to proper data collection. Collected
data were entered into an Excel 2010
data sheet. After data had been cleaned,
they were analysed by using SPSS
version 23 statistical software. Initially a
univariate analysis was conducted and
on selected variables a bivariate analysis
was conducted. The total cost of a clinic
visit was estimated by using the following variables; travelling, lodging
and incidentals.
.
Results
This study employed a Sample size was
335 and response rate was 100%. The
sample consisted of children from seven
districts of Sri Lanka, both gender/sex,
and main ethnic and religious groups.
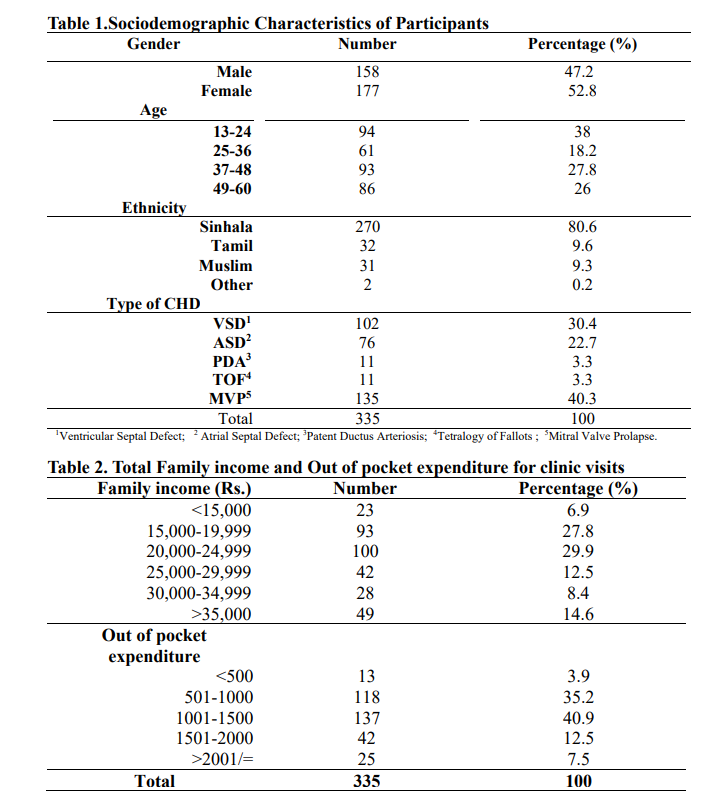
Out of the 335 children who participated
in the study, 47.2% were male (N=158)
and 52.8% were female (N=177).There
was no statistically significant difference
between two genders of participated
children (P>0.05). Ages of the children
varied between 13 months to 60 months
with a mean age of 37.1 months and SD
was 14.5. Majority were in 37 months to
48 months age group (N=93:27.8%).
Majority of the children were Sinhalese
(N=270: 80.6%). There were five types
of congenital heart diseases found in the
study sample .They were; Atrial Septal
Defect (ASD), Ventricular Septal
Defects (VSD), Tetralogy of Fallots
(TOF), Patent Ductus Arteriosis (PDA),
Mitral Valve Prolapse (MVP). Among
them the most common (40.3%)
congenital heart disease was MVP
(N=135).
Total income of the families varied from
Rs.12, 000/= to Rs.80, 000/=
(Mean=Rs.23759.7: SD=Rs.9026.6).
Majority (29.9%) of the families was
included to the total income range
between Rs.20, 000/= to Rs.24, 999/=
(N=100). 23% of participants had taken
support from outside people to attend the
clinic but no one had to pay for them.
80.9% of employed parents could not
attend to work on the clinic day, due to
the clinic visit. 23% of participants lost
their daily income due to the clinic visit.
None of the patients were given
prescriptions to buy drugs from private
pharmacies and none of them had to do
investigations from private laboratories.
All the health care services were
provided by the cardiology clinic of
Sirimavo Bandaranaike Specialized
Children’s Hospital. None of the
participants had an insurance cover to reimburse the expenses of the clinic visit.
23% of children had withdrawn their
savings to cover the expenses and 11
families had borrowed money from
friends and relations.
Discussion
The study sample consisted of children
from seven districts. Majority was from
the central province. Although there was
a female predominance in the study
sample, according to the statistics the
Male: Female ratio of the population of
Sri Lanka was 47.1: 52.9 in 2012/13 ).Data mentioned in the study sample
approximately overlap with this
information. According to the population
statistics there was a Sinhala Buddhist
predominance identified in the districts
which were included to the study. There
were 80.6% of Sinhalese and 81.8% of
Buddhists in the study sample
(6).
According to the study done in year 200
by Ariane J. Marelli et al., 52% of
congenital heart disease children were
females. Majority of the Congenial Heart
Disease children had Ventricular septal
Defects and the second commonest
disease was Atrial Septal Defect
(7).
Mitral Valve prolapse was not
considered in most of the studies but
patients born with Mitral valve prolapse
had abnormal heart sounds and therefore
they were followed up at clinics for 2-3
years. At the end they were reassured
and discharged from the clinic after
prescribing prophylactic antibiotics only
for necessary situations. During this
period of clinic visits, many
opportunities for expenses were
generated. Therefore significant
attention was paid on mitral valve
prolapse during this study, although
clinically not serious.
According to the mean income of a
family, four main social classes were
identified by the Senses and Statistics
Department of Sri Lanka. They are very
poor, poor, middle and rich(8). Mean
income of the poor social class was
Rs.15, 760/= and the mean of the middle
class income was Rs.32, 590/=.
According to the present study mean of
the monthly income was Rs. 27,759/=.
So the mean income of this study falls
between the mean income of poor and
middle social classes. And in the present
study, most of the mothers were
educated up to GCE O/L. In the present
study, there were no children
representing the rich social class. This observation generates two hypotheses;
either CHD is not present in this social
class or they are not attending the
government health care institutions for
services.
According to the study done in 2015 in
India, majority of the Congenital Heart
Disease patients are from the upper
middle class (43%) and lower middle
class (37.5%) families(9). Majority of
patients of the present study also
represented middle and poor social
classes. At the Indian context, family
expenses due to hospitalization for
surgeries to correct Congenital Heart
Disease were studied and it was
calculated as 0.93% of their annual
family income. A median of 15 working
days was missed annually due to
hospitalization. In the present study 80.9
% of participants had missed working
days due to clinic visits. Majority had
managed their expenses within their
monthly income. But in India, Majority
(96.1%) had to depend on other external
sources to cover up their expenses
There is an opportunity of calculating the
non-medical out of pocket expenses of
patients who had undergone corrective
cardiac surgeries. Calculating the nonmedical expenses during the period of
preparing for surgeries and during the
period of hospital stay can be done by
using the ‘Review diary method’
practiced in USA (10). Generally there
are limitations for leading a normal life
after undergoing a cardiac surgery. The
impact of those conditions should be
evaluated by using a validated technique.
Conclusion/Recommendations
Majority were Sinhala Buddhists from
the central province and they showed a
slight female predominance. Among
congenital heart diseases Mitral Valve
Prolapse showed the highest prevalence.
Average out of pocket expenditure for a single clinic visit was Rs.1246.80
(SD=Rs.650.80) Expenses for transport
and food were highest among out of
pocket expenses.
eople should be directed to do necessary
behavioral changes to minimize the out
of pocket expenses. Reducing the period
of stay at the clinic by allocating a time
and providing an efficient service during that time can be used to minimize the
expenses for food, lodging and transport.
This study can be expanded to calculate
the non-medical out of pocket expenses
when undergoing a corrective surgery.
The psychological effects generated on a
congenital heart disease child when
living with the limitations of life should
be studied in detail.
References
1.Christianson A, Howson CP, Modell B. Global Report on Birth Defects. March
Dimes Birth Defects Found [Internet]. 2006; Available from
2. Tom Lissauer WC. Illustrated Textbook of Paediatrics. 5th ed. Elsevier; 2017. 600
p.
3. Framework S. Prevention and Control of Birth Defects in South-East Asia Region
- strategic framework. World Heal Organ. 2013;
4. Lwanga SK LS 1991. Sample size determination in health studies: A practical
manual. Geneva.: World Health Organization; 1991.
5. Marelli AJ, Mackie AS, Ionescu-Ittu R, Rahme E, Pilote L. Congenital heart
disease in the general population: Changing prevalence and age distribution.
Circulation. 2007;115(2):163–72.
6. Department of Censes and Statistics SL. Demographic And Health Survey 2007.
Colombo; 2009.
7.Central Bank of Sri Lanka. Sri Lanka Socio-economic data. 2016;(June) Available from
8.Statistics D of C and. Census and population and Housing 2012 [Internet].
Colombo; 2012. Available from
9.Raj M, Paul M, Sudhakar A, Varghese AA, Haridas AC, Kabali C, et al. Microeconomic impact of congenital heart surgery: Results of a prospective study from
a limited-resource setting. PLoS One [Internet]. 2015;10(6).Available from
10.DiFazio RL, Vessey JA. Non-medical out-of-pocket expenses incurred by
families during their child’s hospitalization. J Child Heal Care [Internet].
2013;17(3):230–41.Available from